31 year old male s/p MVA with LUQ pain and a splenic laceration.



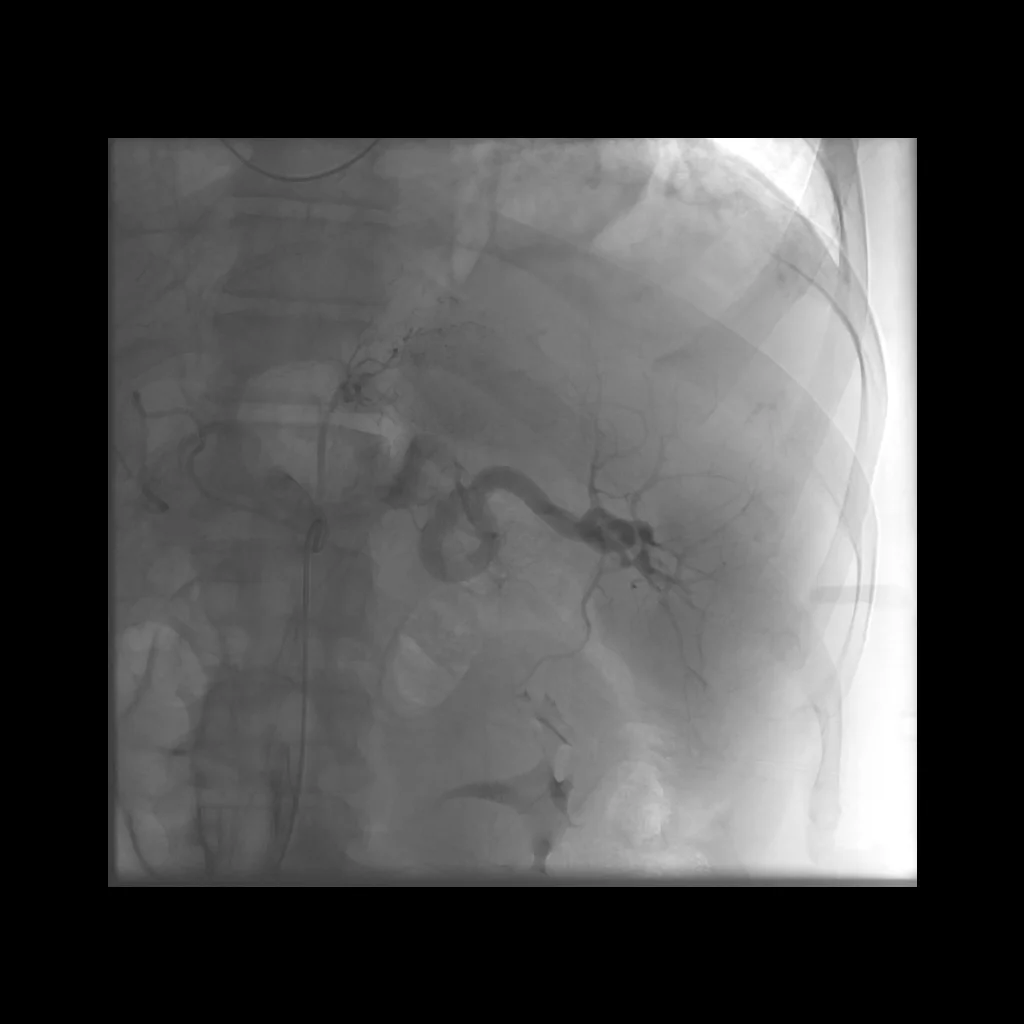




Comment: There are several potential approaches to the endovascular treatment of splenic trauma. In this particular case, we saw a significant perisplenic hematoma on CT and angiography demonstrated active extravasation. While the tortuosity of the main splenic artery made it difficult, it was our goal to navigate the artery and attempt a selective catheterization of the bleeding artery, with the ultimate goal of selective distal embolization. In our opinion, distal embolization is the preferred approach when extravasation is seen. We reserve proximal splenic embolization for when distal embolization is not possible and when active extravasation is not evident on angiography.